Author: ng4mf
An End or a Beginning?
I can honestly say that this class was an awesome experience. Getting to directly work with real patients who have to deal with diseases such as diabetes has been very informing. I came into college interested in working on (specifically) medical robotics. Over the course of time, as I’ve gotten involved with more and more projects, that has begun to change. There are myriad opportunities out there, and there are a lot of different ways they can be solved. Granted, my experience and main interests still lie in embedded systems, but I think talking to real patients helped in forming the understanding that other avenues can be just as interesting or useful (even if the solution is in a different area of expertise). Our particular issue could have been approached from a pharmacological, chemical, electrical, or possibly some other perspective. Perhaps given my background, I usually find an embedded systems application in whatever I am working on. I don’t think that not getting to work with an embedded system would have mattered in the case of this project, though. At the end of the day, what really mattered was that we were trying to figure out ways to help a real person deal with a real problem. Hopefully we’ll be able to keep our group together and pursue this idea further (albeit probably at a much slower pace).
Simulation Vs. The Real Thing
Initially, when we were figuring out ways to test our sensor, we figured that we could simulate sweat by diluting saline solution. We found the average salinity of sweat and knew the salinity of the solution, so we could create a solution that would mimic sweat. We were wrong. First of all, the chemical make up is not the same. As far as I’ve understood it, I think that means that not all salinity values are equal. On a lower level, that makes sense. Different chemicals will have different chemical properties. The thing keeping us back was the “bodily fluids are gross” factor. However, when we started seeing odd results with our saline solution, we came back to the drawing board. It seemed like the initial hope we had had (that sweat and insulin would produce different results) would not be supported. At the same time, we came back around to the idea of testing with actual sweat. It turned out that the real thing was different than the simulant. Honestly, that was something that we should have thought of at the beginning. That is drilled in as we learn the math for our various majors: you can run calculations, but you cannot account for every little possibility.
For the most part, sweat behaved very differently than our simulant. Not only was the conductivity different, but the values for different people varied a lot. For the most part, everyone had a very large voltage reading between the two electrodes that we used (I had a very low reading, but I’m thinking that was more due to volume or some other experimental error that we didn’t notice). The good news was that testing with actual sweat caused a larger discrepancy between ranges of voltage for insulin and sweat, so our thresholds became easier to determine. Long story short, we’ve relearned that you can’t beat real data from real people.
NG
Tunneling
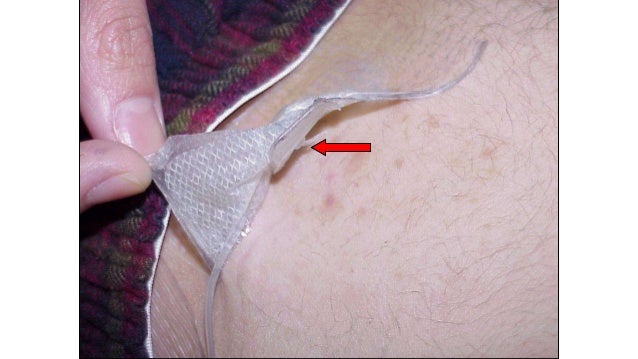
Interestingly enough, we stumbled across a problem that isn’t particularly visible in the literature. Insulin tunneling occurs when some kink in the insulin teflon needle or scar tissue (still figuring out whether it’s real scar tissue or something else) causes insulin to pool on skin. During a recent interview, we discovered that some of the most dangerous pooling occurs when insulin pools underneath the skin (i.e. locally disburses, but doesn’t disburse throughout the entire body system). Initially, I had thought that the pooling only occurred on the outside of the skin. This second form of pooling is actually more dangerous than the first, because it is virtually impossible to remove the locally disbursed insulin, and eventually that insulin will hit the body, which might coincide with a bolus, causing a blood sugar low.
The solution we were examining was aimed at detecting insulin on the surface of the skin. However, upon thinking about it, I can’t seem to come up with a solution to the internal pooling issue. Electrodes can’t be used on the tip of the needle because the insulin would touch the electrode regardless of whether it was pooling or not as it was released by the pump. However, I might be underestimating the changes that insulin causes in the locality in which it is distributed. Additionally, the patient stated that they were unsure about which type of tunneling occurred more often. However, the patient seemed very interested in the idea of tunneling detection. For now, I believe our group will proceed with the method we had initially thought about, but internal tunneling is definitely an issue that we will need to revisit and brainstorm about to come up with possible solutions.
For reference, I’ve included a picture of internal tunneling. In the picture, the insulin can be seen, which is not always the case with tunneling. Part of the problem is that tunneling is hard to detect, but that is also what makes it an important and significant engineering challenge.
-N
Personal Health
For this class period, I have been trying to figure out how to keep doing all the things I’m involved with while sleeping better. I’ve always known that I start losing productivity at some point in the day, but generally I ignore tiredness (or drink coffee) so as to get something done. This compounds over time, because I wake up more tired the next day and have a similar workload, meaning I’ll be even less efficient than the first day; it’s kind of like a productivity-loss cycle. Today I tried to go to bed early and wake up early, but as happens almost every time I try that, I woke up much later than I intended. I still woke up early enough to do the work I had intended to complete for class, but there were some other things I’d been trying to do that I won’t have time for now. Something that might be worth considering is taking a nap in the evening. I’ve normally avoided naps because it takes me a while to fall asleep, but maybe the idea is worth revisiting. I’ll also be talking to my partner and see what suggestions he has to make, and go from there. Hopefully we can figure out something that can be maintained beyond J-Term, I really enjoy most of the things I work on, but I’ve come to the realization that I also enjoy sleep.
-Neeraj
January 5, 2016
Somehow my first post ended up on a new website instead of linked here. See original here.
Copy of text:
The interview process today was very illuminating. I came in not having any idea what living with the conditions that the patients are living with was like. The constant care that they have to take in order to remain active seems like a very difficult, and likely mentally exhausting, task. This provided some perspective on why I became interested in embedded systems applications in the medical sphere in the first place.
One of the most interesting insights that seems obvious when said but did not initially occur to me was that the monitoring equipment is invasive. It comes with a whole host of side effects such as rashes and calluses. The devices can be cumbersome and risky, resulting in people not wanting to always use them. One of the patients stated that for diabetes, the patient could take better care of himself or herself when using shots instead of insulin pumps. This seems to indicate the need for a noninvasive method by which to measure blood glucose, or at the very least a noninvasive way by which to indicate whether blood glucose has crossed a high/low threshold that requires intervention to prevent a bad reaction.
-Neeraj

{kind=link}
{kind=link}